Brown, commonly known as “the Berlin patient,” was cured of HIV whenever he underwent a bone marrow transplant in 2007 to treat leukemia, which he individually had. The donor had a genetic mutation called “CCR-delta 32” that made him resistant to HIV to the point of near resistance. Whenever Brown received the transplant, that someone had handed genetic resistance down to him.
As per the US Centers for Disease Control and Prevention (CDC), Americans pay 14% of their total prescription drug costs out from pocket every year, plus the United States spends more per capita on over the counter drugs compared to any other high-income country in the world. High expenses lead to a specific magnitude of nonadherence among patients generally. Still, little information exists in regard to the impact of monetary barriers on adherence if anyone is coping with HIV specifically.
New HIV Resource on Amazon get your copy today.
A study presented inside the CDC’s Morbidity and Mortality Weekly Report indicates from 2016-17, 14% of people coping with HIV have been using a drug-cost saving strategy, and 7% have received cost saving-related nonadherence. The CDC’s Medical Monitoring Project analyzed nationally representative surveillance data on health care bills, behaviors, and clinical outcomes among adults with HIV infection. Data were collected through medical record abstraction and also in-person and telephone interviews between June 2016-May 2017. Investigators weighted data for unequal selection probabilities and nonresponse. Analyzing statistics from 3948 people taking pharmaceuticals, the prevalence of prescription drug cost-saving strategies among those living with HIV was estimated overall, it is not excellent sociodemographic characteristics. Investigators also assessed differences in clinical outcomes between individuals who did and not having cost-saving related nonadherence. Questions pertained to 6 several types of cost-saving strategies. Patients reported anytime they had asked a clinician and got a lower-cost medication, used alternative therapies, bought prescription drugs from another country, skipped doses, taken less medication, or delayed filling a prescription on account of cost. Those interviewed were asked concerning prescription drugs, not solely antiretrovirals. Cost-saving nonadherence was qualified by having ordered cost-saving strategies of skipping doses, taking less medication, or delaying a prescription only because of cost. Care engagement and viral suppression were abstracted from medical records. Individuals interviewed were also asked whenever they needed but had not received medication that is caused by the Ryan White AIDS Drug Assistance Program (ADAP) to research unmet needs. Of the approximately 14% of Americans with HIV who had used a medication cost-saving strategy, 4% had skipped doses, 4% took less medicine, and 6% had delayed a prescription. In the categories should have the tanks not considered directly nonadherent, 9% had asked clinicians for lower-cost medicine, 1% had bought medication from another country, and 2% used alternative medicine. Household income above the poverty line was associated with nonadherence as a consequence of prescription drug costs, with 8.3% reporting nonadherence above the poverty line ($12,490 as of 2019) concerning 5.3% of your desired poverty line. “Persons with incomes above the poverty level may not be eligible for the Ryan White HIV/AIDS Program as well as assistance programs that can reduce medication costs,” the authors of a given report wrote. Individuals that reported the unmet necessity of medication through ADAP were around five times most likely nonadherent as a consequence of cost than individuals that received ADAP. People coping with HIV who reported cost-saving related nonadherence were more unlikely to become virally suppressed some knowledge newest viral load test (64%) than individuals who did not report cost-saving related nonadherence (76%). Nonadherence regarding drug cost was also connected with lower HIV care engagement rates and a lot more emergency department visits. The more occurrence of costly hospitalizations and lower viral suppression rates (increasing likelihood of HIV transmission) among those who were nonadherent as a consequence of prescription drug costs demonstrate that cost-related nonadherence provides broad social needs with several stakeholders. Inside a recent interview concerning upcoming long-acting antiretroviral therapies, Carlos del Rio, MD, FIDSA, Co-director regarding the Emory Center for AIDS research, claimed that clinicians must take cost seriously when treating HIV.
The Trump administration announced last week a brand new program that will provide HIV prevention medications without charge for uninsured patients. This pre-exposure prophylaxis (or PrEP) drugs are effective in preventing HIV, but with a cost of $2,000 a month, they’re far too expensive for people without insurance. This new program will provide PrEP at no cost for as much as 200,000 uninsured patients. Supporters have lauded this move being a significant step toward President Trump’s intention to end HIV in the United States. Others have criticized it as not going far enough: They would rather the govt expedite generic drug production and lower the price of PrEP. AD Both are missing an important point: Free or reduced-cost drugs may have no impact if patients can’t access them. The rural South is a growing epicenter for HIV, but as the South makes up about most new HIV diagnoses, it has a quarter of all PrEP-providing clinics. In West Virginia, only 27 percent of the state’s rural counties offer any HIV prevention services. In North Carolina, just two considering the state’s 85 local health departments reported to researchers last year they prescribed PrEP. In Mississippi, patients have taken to bring in three or more hours to access the one health center that dispenses 80 percent of all PrEP pills within the state. And that’s when the patient knows to question for PrEP. Only half of most uninsured patients have a regular supply of medical care.
Patients are at high risk of contracting HIV are by far less more likely to do so since they often possess by him marginalized communities that have deep distrust considering the medical system. A Centers for Disease Control and Prevention report found that while African Americans account for 44 percent of individuals who would be eligible for PrEP, they make up for only 11 percent among those on PrEP. African American men who have sex with men possess a 1-in-2 lifetime risk of contracting HIV, yet it includes only 26 percent on PrEP (in comparison with 42 percent of the white peers). Without concerted outreach efforts to these vulnerable communities, the promise of free drugs won’t translate to patients taking them.
The administration’s new program covers only medications themselves. The medical appointment to get the prescription isn’t covered, nor are lab tests or ongoing care. CDC guidelines require that patients undergo multiple blood tests before starting PrEP, and after that, regular testing every three months while on it. Regarding the uninsured, these tests cost hundreds of dollars a year and can price patients from PrEP care. Versus giving free medications to certain uninsured people, a more exceptional solution is helping these patients get health insurance. Medicaid already covers 42 percent of adults with HIV (in comparison with 13 percent of the general adult population), and patients on state Medicaid programs receive coverage not only for PrEP and HIV drug therapies but other comprehensive services such as lab testing, care coordination, and community-based services. Admittance to these public insurance programs is essential for prevention. The federal Ryan White program, which funds cities and states to care for low-income people with HIV, supports only those already diagnosed with HIV. It does not help individuals who could be prevented from getting HIV and does not cover PrEP. Expanding Medicaid to those at high risk for HIV would allow them to receive PrEP and insurance for it the other services they need.
Patients also need more places to access HIV prevention and treatment. An integral access point is clinics funded by the Title X family planning program. Of the 4,000 Title X clinics throughout the country, 90% provide HIV testing, and a third offer PrEP. These clinics serve low-income patients in rural and underserved areas but now are threatened with closure because of Trump administration’s new Title X restrictions. When the Trump administration wants to achieve its aim of eradicating HIV, it is required to end harmful policies for example the Title X gag rule. And instead of dismantling the Affordable Care Act, it should support state-based Medicaid expansion. It is required to remove discriminatory policies for example the conscience rule and the public charge rule that further stigmatize LGBTQ, minority and immigrant populations that already face the best barriers to care. The Trump administration’s free medication program distracts from the real challenges of HIV prevention and treatment. Pills are no panacea when patients can’t access them in the first place, and after that can’t afford the rest of the health care which comes besides treatment. The administration has got the power to fulfill its promise to end the HIV/AIDS epidemic, but it must start with an honest study of its existing policies. Otherwise, it will keep making tiny steps forward against a backdrop of giant steps backward.
Although HIV/AIDS has mainly faded from the headlines, the disease continues to be infecting millions. When looking at the United States, about 1.1 million people age 13 and older are living with HIV, the virus which causes AIDS, according to the Centers for Disease Control and Prevention. A decade ago, the sheer number of U.S. infections was declining substantially every year, but that stopped in 2013. Since that time, about 39,000 individuals have become newly infected each year, which prompted the CDC this present year to declare the nation’s progress in preventing HIV has stalled. Current commentary by four top public health insurance and AIDS experts, published within the New England Journal of Medicine, reports that a lot more than two-thirds of new infections occur those types of who will be poor or who are ethnic, racial or sexual minorities. The CDC did note locales which have enacted plans to eliminate HIV epidemics within their communities have observed some success in prevention, with new HIV infections down 40 percent in Washington, D.C., and 23 percent in New York City from 2010 to 2016. No cure exists for HIV or AIDS. (AIDS itself will not kill; nonetheless, it allows other diseases to kill.) Nearly 16,000 people into the United States diagnosed with HIV died in 2016, the newest data available. However, antiretroviral therapy — an HIV treatment regimen that has been introduced into the mid-1990s — can keep HIV controlled, preventing it from progressing to AIDS. Individuals who begin this treatment early and take it regularly as recommended can reduce, and possibly eliminate, their odds of transmitting HIV to others and generally can live long healthy lives.
The possibility of passing in the HIV virus is wholly eradicated by successful drugs treatment; a landmark study has revealed, in a substantial boost towards the prospects of ceasing the AIDS epidemic.
Research of about 1,000 gay male couples with one partner with HIV who had taken antiretroviral therapy (ART) discovered no new cases of transmission towards the HIV-negative partner during sex without a condom.
During the period of the eight-year study, 15 men were infected with HIV, the herpes virus, which causes AIDS. However, genetic tests revealed that the transmissions were a result of the HIV-negative men having sexual relations with someone aside from their partner.
The report, in The Lancet medical journal, indicates that using ART to suppress HIV to undetectable levels showed that it was incapable of transmission during sex.
If everyone in the world with HIV knew their status and had usage of successful treatment, no new cases would occur, the study suggests.
The United Nations has established a target of ceasing the global HIV/AIDS epidemic by 2030.
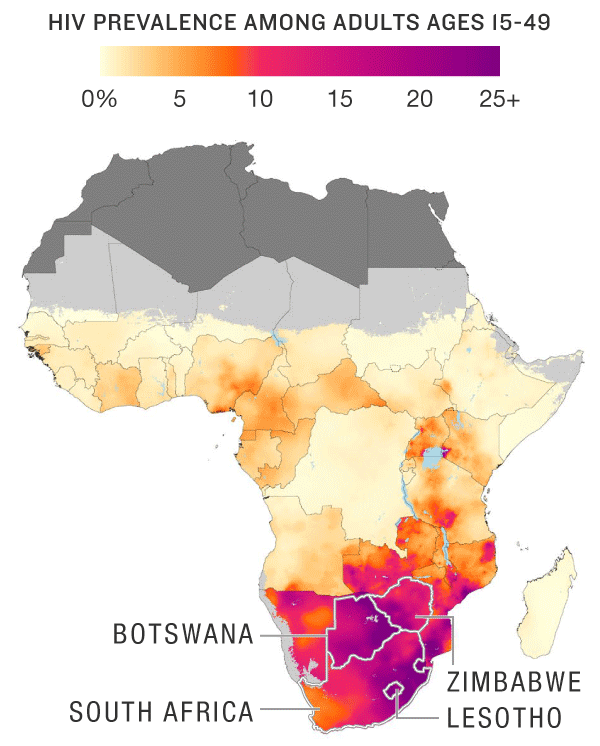
The tide, in other areas, is slowly turning in southeastern Africa — which involves international locations like South Africa, Mozambique, Lesotho and Botswana — and which remains the epicenter associated with the epidemic and home to over fifty percent the 36.9 million people living with the disease. The rates of fatalities and infections one can find declining overall. However, a July 2018 report through the United Nations’ AIDS agency found a $5.4 billion shortage in international financing needed to accomplish ultimate triumph.
A first-of-its-kind new map can help boost the precision associated with HIV/AIDS response as some data-savvy scientists narrow their focus on the continent’s worst-affected areas — into the size of a tiny town.
Research published presents what these scientists explain as the most step-by-step map ever produced of HIV prevalence across sub-Saharan Africa. The group behind the map is a global consortium of epidemiologists led by the University of Washington-Seattle’s Institute for Health Metrics and Evaluation. Their work appears when looking at the peer-reviewed journal Nature.
The researchers do not just go country by country. Researchers break down the continent into a grid of tens and thousands of 9.6-square-mile squares. The effect is a view of HIV distribution that is more fine grain compared to general national or province level statistical data, and that could have a significant effect on how resources are assigned to diagnose, treat and stop new infections.
Reference
Fan, Yaxin, Xinyan Zhu, et al. “Network-Constrained Spatio-Temporal Clustering Analysis of Traffic Collisions in Jianghan District of Wuhan, China.” PLoS One, vol. 13, no. 4, Public Library of Science, Apr. 2018, p. e0195093.